Introduction
The anatomy of the wrist joint is extremely complex, probably the most complex of all the joints in the body. The wrist is actually a collection of many bones and joints. These bones and joints let us use our hands in lots of different ways. The wrist must be extremely mobile to give our hands a full range of motion. At the same time, the wrist must provide the strength for heavy gripping.This guide will help you understand
- what parts make up the wrist
- how those parts work together
Important Structures
The important structures of the wrist can be divided into several categories. These include
- bones and joints
- ligaments and tendons
- muscles
- nerves
- blood vessels
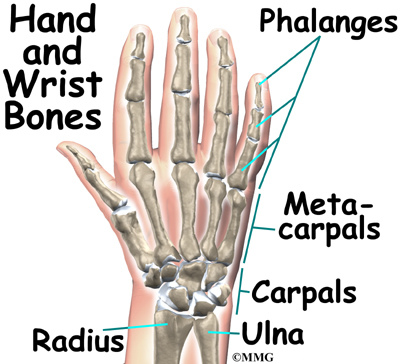
Bones and JointsThere are 15 bones that form connections from the end of the forearm to the hand. The wrist itself contains eight small bones, called carpal bones. These bones are grouped in two rows across the wrist. The proximal row is where the wrist creases when you bend it. Beginning with the thumb-side of the wrist, the proximal row of carpal bones is made up of thescaphoid, lunate, and triquetrum. The second row of carpal bones, called the distal row, meets the proximal row a little further toward the fingers. The distal row is made up of the trapezium, trapezoid, capitate, hamate, and pisiform bones.The proximal row of carpal bones connects the two bones of the forearm, the radius and the ulna, to the bones of the hand. The bones of the hand are called the metacarpal bones. These are the long bones that lie within the palm of the hand. The metacarpals attach to the phalanges, which are the bones in the fingers and thumb.
One reason that the wrist is so complicated is because every small carpal bone forms a joint with the bone next to it. This means that what we call the wrist joint is actually made up of many small joints.
Articular cartilage is the material that covers the ends of the bones of any joint. Articular cartilage can be up to one-quarter of an inch thick in the large, weight-bearing joints. It is thinner in joints such as the wrist that don't support a lot of weight. Articular cartilage is white, shiny, and has a rubbery consistency. It is slippery, which allows the joint surfaces to slide against one another without causing any damage.
The function of articular cartilage is to absorb shock and provide an extremely smooth surface to make motion easier. We have articular cartilage essentially everywhere that two bony surfaces move against one another, or articulate. In the wrist, articular cartilage covers the sides of all the carpals and the ends of the bones that connect from the forearm to the fingers.
Ligaments and Tendons
Ligaments are soft tissue structures that connect bones to bones. The ligaments around a joint usually combine to form ajoint capsule. A joint capsule is a watertight sac that surrounds a joint and contains lubricating fluid called synovial fluid. In the wrist, the eight carpal bones are surrounded and supported by a joint capsule.
Two important ligaments support the sides of the wrist. These are the collateral ligaments. There are two collateral ligaments that connect the forearm to the wrist, one on each side of the wrist.
As its name suggests, the ulnar collateral ligament (UCL) is on the ulnar side of the wrist. It crosses the ulnar edge (the side away from the thumb) of the wrist. It starts at the ulnar styloid, the small bump on the edge of the wrist (on the side away from the thumb) where the ulna meets the wrist joint. There are two parts to the cord-shaped UCL. One part connects to the pisiform (one of the small carpal bones) and to the transverse carpal ligament, a thick band of tissue that crosses in front of the wrist. The other goes to the triquetrum (a small carpal bone near the ulnar side of the wrist). The UCL adds support to a small disc of cartilage where the ulna meets the wrist. This structure is called the triangular fibrocartilage complex (TFCC) and is discussed in more detail below. The UCL stabilizes the TFCC and keeps the wrist from bending too far to the side (toward the thumb).
The radial collateral ligament (RCL) is on the thumb side of the wrist. It starts on the outer edge of the radius on a small bump called the radial styloid. It connects to the side of the scaphoid, the carpal bone below the thumb. The RCL prevents the wrist from bending too far to the side (away from the thumb).
Just as there are many bones that form the wrist, there are many ligaments that connect to and support these bones. Injury or problems that cause these ligaments to stretch or tear can eventually lead to arthritis in the wrist.
At the wrist, the end of the ulna bone of the forearm articulates with two carpal bones, the lunate and the triquetrum. A unique structure mentioned earlier, the triangular fibrocartilage complex (TFCC), sits between the ulna and these two carpal bones. The TFCC is a small cartilage pad that cushions this part of the wrist joint. It also improves the range of motion and gliding action within the wrist joint.
There are several important tendons that cross the wrist. Tendons connect muscles to bone. The tendons that cross the wrist begin as muscles that start in the forearm. Those that cross the palm side of the wrist are the flexor tendons. They curl the fingers and thumb, and they bend the wrist. The flexor tendons run beneath the transverse carpal ligament (mentioned earlier). This structure lies on the palm side of the wrist. This band of tissue keeps the flexor tendons from bowing outward when you curl your fingers, thumb, or wrist. The tendons that travel over the back of the wrist, the extensor tendons, run through a series of tunnels, called compartments. These compartments are lined with a slick substance called tenosynovium, which prevents friction as the extensor tendons glide inside their compartment.
Muscles
The main muscles that are important at the wrist have been mentioned above in the discussion about tendons. These muscles generally start further up in the forearm. The tendons of these muscles cross the wrist. They control the actions of the fingers, thumb, and wrist.
Nerves
All of the nerves that travel to the hand cross the wrist. Three main nerves begin together at the shoulder: the radial nerve, the median nerve, and the ulnar nerve. These nerves carry signals from the brain to the muscles that move the arm, hand, fingers, and thumb. The nerves also carry signals back to the brain about sensations such as touch, pain, and temperature.
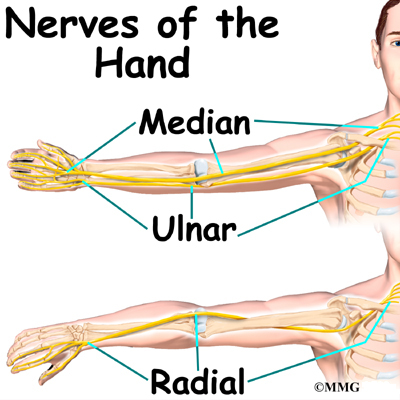
The radial nerve runs along the thumb-side edge of the forearm. It wraps around the end of the radius bone toward the back of the hand. It gives sensation to the back of the hand from the thumb to the third finger. It also goes to the back of the thumb and just beyond the main knuckle of the back surface of the ring and middle fingers.The median nerve travels through a tunnel within the wrist called the carpal tunnel. The median nerve gives sensation to the palm sides of the thumb, index finger, long finger, and half of the ring finger. It also sends a nerve branch to control thethenar muscles of the thumb. The thenar muscles help move the thumb and let you touch the pad of the thumb to the tips each of each finger on the same hand, a motion called opposition.The ulnar nerve travels through a separate tunnel, called Guyon's canal. This tunnel is formed by two carpal bones (thepisiform and hamate), and the ligament that connects them. After passing through the canal, the ulnar nerve branches out to supply feeling to the little finger and half the ring finger. Branches of this nerve also supply the small muscles in the palm and the muscle that pulls the thumb toward the palm.The nerves that travel through the wrist are subject to problems. Constant bending and straightening of the wrist and fingers can lead to irritation or pressure on the nerves within their tunnels and cause problems such as pain, numbness, and weakness in the hand, fingers, and thumb.Blood VesselsTraveling along with the nerves are the large vessels that supply the hand with blood. The largest artery is the radial arterythat travels across the front of the wrist, closest to the thumb. The radial artery is where the pulse is taken in the wrist. Theulnar artery runs next to the ulnar nerve through Guyon's canal (mentioned earlier). The ulnar and radial arteries arch together within the palm of the hand, supplying the front of the hand and fingers. Other arteries travel across the back of the wrist to supply the back of the hand and fingers.
Causes
What causes a scaphoid fracture?
A scaphoid fracture is almost always caused by a fall on the outstretched hand. We commonly try to break a fall by putting our hands out for protection. Landing on an outstretched hand makes hand and wrist injuries, including a fracture of the scaphoid bone, fairly common.
When a scaphoid fracture is recognized on the first X-ray, treatment begins immediately. But patients often assume that the injury is just a sprain, and they wait for it to heal on its own. In some cases, the wrist gets better. In many cases the bone fails to heal. The scaphoid fracture then develops into what surgeons call a nonunion.
A nonunion can occur in two ways. In a simple nonunion, the two pieces of bone fail to heal together. The second type of nonunion is much more serious. The lower half of the fractured bone loses its blood supply and actually dies. This condition is called avascular necrosis (Avascular means no blood supply, and necrosis means dead.)
The scaphoid bone is at risk for avascular necrosis. Only one small artery enters the bone, at the end that is closest to the thumb. If the fracture tears the artery, the blood supply is lost. Avascular necrosis becomes easy to see on X-rays several months after the injury.
Symptoms
How will I know if I have a scaphoid fracture?
The symptoms of a fresh fracture of the scaphoid bone usually include pain in the wrist and tenderness in the area just below the thumb. You may also see swelling around the wrist. The swelling occurs because blood from the fractured bone fills the wrist joint. Thin people will see a bulging of the joint capsule. The joint capsule is the watertight sac that encloses the joint.
Symptoms of a nonunion of the scaphoid bone are more subtle. You may have pain when you use your wrist. However, the pain may be very minimal. It is fairly common for doctors to see a nonunion of the scaphoid bone on X-rays, but the patient can't remember an injury. These people probably suffered a wrist injury years ago that they thought was a simple sprain. Still, the most common symptom of a nonunion is a gradual increase in pain. Over several years the nonunion can lead to degenerative arthritis in the wrist joint.
Diagnosis
What tests will my doctor run?
Your doctor will first take a medical history. You will be asked questions about your pain and about any injuries to your wrist. Your doctor will also do a physical exam. The prodding and moving may hurt your wrist a bit. But it is important that your doctor know exactly where your pain is coming from.
Doctors should assume that any patient who has fallen on an outstretched hand and has swelling or tenderness on the thumb side of the wrist has a scaphoid fracture. You should assume this until tests prove otherwise. X-rays taken immediately after the injury may not show a fracture. Still, most surgeons will put a cast on the wrist and get another X-ray in 10 days. This gives the edges of the fractured bone time to heal, and may prevent nonunion. By waiting 10 days, the fracture is easier to see on an X-ray.
If it is still not clear whether or not you have a fracture, your doctor may order other imaging tests. You may have a bone scan done. A bone scan involves injecting tracers into your blood stream. The tracers then show up on special X-rays of your wrist. The tracers build up in areas of extra stress to bone tissue, such as a fracture.
Your doctor may also order a magnetic resonance imaging (MRI) scan. An MRI scan is a special imaging test that uses magnetic waves to create pictures of your body in slices. The MRI scan shows tendons as well as bones. It is painless and requires no needles or injections
Treatment
Can a fracture or nonunion be healed?
Nonsurgical Treatment
Fracture
If the fracture is identified immediately and is in good alignment, you will probably wear acast for nine to 12 weeks. The cast will cover your forearm, wrist, and thumb. This is necessary to hold the scaphoid bone very still while it heals. Your doctor will take X-rays at least once a month to check the progress of the healing. Once your doctor is sure the fracture has healed, the cast will be removed. Even with this type of treatment, there is still a risk that the fracture may not heal well and will become a nonunion.
Nonunion
A fracture that doesn't heal within several months is considered a nonunion. If the injury is fairly recent, your doctor might recommend more time in the cast. He or she might also prescribe an electrical stimulator. The electrical stimulator is a device that sends a small electrical current to your scaphoid bone. You wear it like a large bracelet for 10 to 12 hours a day. Electrical current has been shown to help the bones heal.
Surgery
Screw Fixation
Some surgeons report good results doing surgery right away when a patient has had a recent, nondisplaced scaphoid fracture. Studies have shown that this method can help people get back to activity faster than wearing a cast for up to 12 weeks. The procedure involves inserting a screw through the scaphoid. The screw holds the scaphoid firmly until it heals.
Scaphoid Debridement
In cases where a nonunion has occurred depite wearing a cast and using an electrical stimulator, surgery will likely be suggested. An incision is made in the wrist directly over the scaphoid bone. The surgeon finds the old fracture line on the scaphoid bone. All the scar tissue between the two halves of the bone must be removed (debrided). This creates a fresh bone surface to allow healing to begin again. In some cases, damaged bone tissue from the scaphoid is also removed.
Bone Graft Method
Your surgeon may use a bone graft. A bone graft involves taking bone tissue from another spot in your wrist and inserting it into the fracture. A bone graft can stimulate healing on the surface of the bones. The bone graft is usually taken through a second small incision just above the wrist. (It is sometimes taken from the pelvis, through an incision in the side of your hip.)
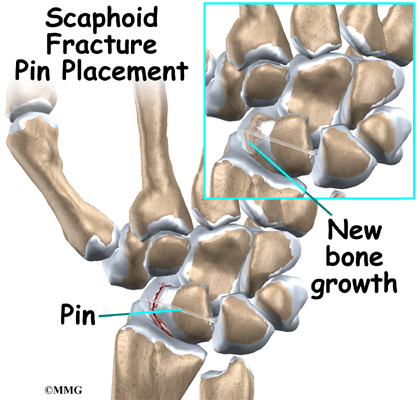
After the bone graft is placed between the parts of the scaphoid bone, some surgeons also insert a metal pin or screw across the bone. The goal is to hold the two pieces of bone tightly together, allowing them to fuse into one bone.
When the surgery is complete, the incision is stitched closed. The arm is placed in a large bandage or a splint. You are then awakened and taken to the recovery room.
Sometimes the bones still do not heal as planned. Surgeons call a fused bone that fails to heal a pseudarthrosis. If the nonunion continues to cause pain, you may need a second operation. Your surgeon will probably add more bone graft and check that the pins or screws are holding the bones together.
Rehabilitation
What will my recovery be like?
Nonsurgical Rehabilitation
If the bone is in good alignment, and there are no problems with the blood supply to the bone, you may be placed in a cast for nine to 12 weeks. Some doctors prefer to start with a long-arm cast. Others use a thumb-spica cast designed to keep the wrist and thumb from moving.
The amount of time you need to wear the cast depends on what part is fractured and whether the bones heal well. When your doctor is certain the bones have healed, your cast will be removed. Your wrist will probably be stiff and weak from being in the cast. You may need physical or occupational therapy to help improve wrist range of motion and strength.
After Surgery
Depending on the type of surgery you have, you may be placed in a splint for up to 12 weeks after surgery. Your surgeon will X-ray the wrist several times after surgery to make sure that the bones are healing properly. Once the two halves of the scaphoid bone have healed, you can safely begin a rehabilitation program.
You may need physical or occupational therapy sessions for six to eight weeks after surgery. The first few treatments will focus on controlling the pain and swelling. You will work into doing exercises to help strengthen and stabilize the muscles around the wrist joint. Other exercises are used to improve fine motor control and dexterity of your hand. You'll be given tips on ways to do your activities while avoiding extra strain on the wrist joint.
|
|
|


















